1. Introduction#
“We make our world significant by the courage of our questions and the depth of our answers.”
— Carl Sagan, in Cosmos (Chapter 12), 1980.
This chapter starts with the clinical background, followed by the challenges in the treatment process. Next, it discusses the unmet clinical needs, and ends with the research hypothesis and the structure of the thesis. Chapter 2 explains the radiotherapy workflow and the AI concepts used throughout. The research chapters then proceed by theme: dosimetric awareness and clinical need in Part One, the sensitivity of dose-prediction models in Part Two, and the robustness of segmentation models in Part Three.
Clinical Background#
Glioblastoma, also known as Glioblastoma Multiforme (GBM), is the most common and aggressive primary malignant brain tumour in adults [Tan et al., 2020], with an incidence of about 3 per 100,000 [Gramatzki et al., 2016, Ostrom et al., 2020]. It was first recorded in 1800 and named in 1926 by Percival Bailey and Harvey Cushing, with “multiforme” describing its varied appearance due to necrosis (tissue death), bleeding, and cysts [Stoyanov and Dzhenkov, 2018]. The World Health Organization (WHO) classifies GBM as a Grade IV astrocytoma, marked by fast growth, widespread invasion, and a tendency for necrosis and angiogenesis (new blood vessel formation to support tissue growth) [Louis et al., 2021]. GBM makes up 14.6% of all primary brain and Central Nervous System (CNS) tumours, 48.3% of primary malignant brain tumours, and 57.3% of all gliomas in adults [Andreatta et al., 2020]. It is more common in males than females and the mean age at diagnosis is between 59 and 62 years [Gramatzki et al., 2016], with incidence increasing significantly to 15.24 per 100,000 between ages 75 to 84 [Alexander and Cloughesy, 2017].
GBMs are divided into two main types: primary (de novo) and secondary (progressive). Primary GBM appears suddenly without a prior lesion, usually affects older patients (average age of 62 years), and makes up about 95% of cases. Secondary GBMs develop from lower-grade gliomas, typically occur in younger patients (average age of 45 years), and represent around 5% of cases [Lim et al., 2011]. The Isocitrate Dehydrogenase (IDH) mutation status is an important molecular marker for GBM classification. According to the 2021 WHO classification [Louis et al., 2021], IDH-mutant astrocytomas (previously called secondary GBMs) are distinct from IDH-wildtype GBMs, as they have different outcomes. Patients with IDH-mutant tumours generally live longer than those with IDH-wildtype GBMs [Sarac et al., 2025].
Motivation: Glioblastoma Treatment#
Managing GBM in clinical practice is difficult due to its complex nature. GBM shows significant differences within and between tumours at the genetic, molecular, and cellular levels [Sottoriva et al., 2013]. These tumours have varied genetic mutations and molecular profiles, which result in different physical traits and responses to treatment [Verhaak et al., 2010]. This variation affects imaging features, such as differences in contrast enhancement, oedema, and necrosis seen on Magnetic Resonance Imaging (MRI) scans [Ellingson et al., 2015]. These differences make it hard to monitor tumour behaviour and growth patterns, which impacts treatment outcomes and complicates the development of effective therapies.
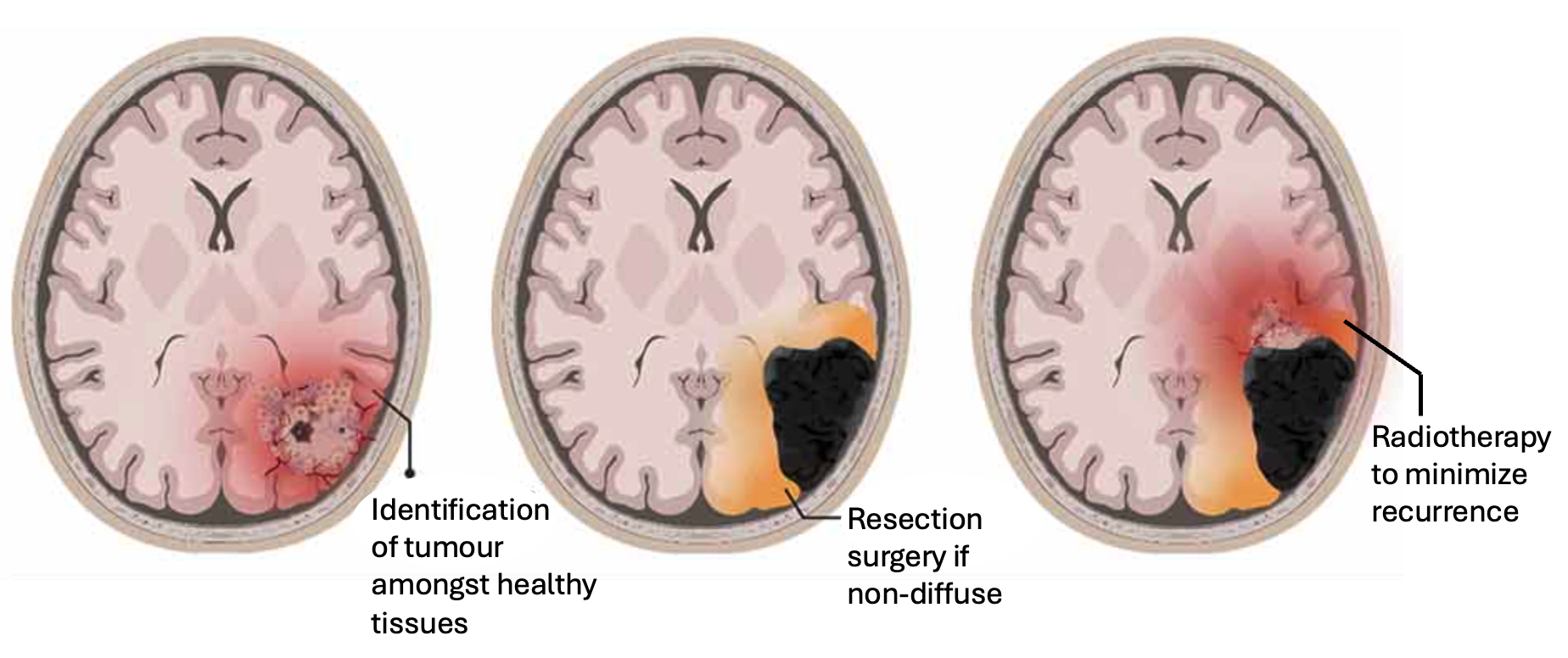
Standard-of-care treatment for GBM relies on identification of tumour boundaries, maximally resecting it, and then performing post-operative Radiotherapy (RT) to target residual microscopic extensions of the tumour cells at the boundaries of the resection area. Figure adapted from [Hills et al., 2022].#
Standard-Of-Care: The standard treatment for GBM, known as the “Stupp protocol”, involves a combination of methods. It includes maximal safe surgical removal of the tumour, followed by RT and chemotherapy with temozolomide [Stupp et al., 2005]. This approach aims to extend survival and enhance the quality of life for patients with GBM. The treatment consists of the following components:
Surgical Resection is the first and most important step in treating GBM. The main goals are to collect tissue for diagnosis and to reduce the tumour size while protecting brain function [De Witt Hamer et al., 2012]. Research shows that removing more of the tumour improves overall survival and delays disease progression [Sanai et al., 2011]. Advanced tools, such as intraoperative MRI [Senft et al., 2011], neuro-navigation systems [Orringer et al., 2012], and fluorescence-guided surgery with 5-Aminolevulinic Acid (5-ALA) [Stummer et al., 2006], help surgeons achieve the maximum safe removal of the tumour. However, complete removal is often not possible because the tumour spreads into surrounding brain tissue.
Postoperative RT is a key part of GBM treatment. Standard external beam RT provides a total dose of 60 Gray (an absorbed dose of 1 Joule/kilogram), given in 2 Gray doses over six weeks, targeting remaining tumour cells and areas with possible microscopic spread [Stupp et al., 2005]. RT significantly increases average survival time compared to surgery alone [Walker et al., 1979]. Methods like Intensity-Modulated Radiotherapy (IMRT) and Stereotactic Radiosurgery (SRS) improve precision, reducing harm to healthy brain tissue [Cho et al., 2010]. Shorter RT schedules are used for elderly patients or those in poor health to lessen treatment time and side effects [Roa et al., 2004]. Artificial Intelligence (AI) is a promising tool to improve RT by aiding in tumour contouring, refining treatment plans, and predicting how well treatment response [Bibault et al., 2016].
Chemotherapy with temozolomide, an oral drug that damages tumour Deoxy-Ribonucleic Acid (DNA), is a key part of GBM treatment. The Stupp protocol [Stupp et al., 2005] showed that using temozolomide alongside RT, followed by six cycles of temozolomide alone, greatly improves average survival and two-year survival rates compared to RT alone. The O6-Methyl Guanine-DNA Methyltransferase (MGMT) promoter’s methylation status predicts how well temozolomide will work, with methylated tumours responding better [Hegi et al., 2005]. However, resistance to temozolomide and tumour recurrence are major issues, leading to research on new drugs and combined treatments [Frosina, 2009].
Dismal Prognosis and its Causes: Despite improvements in diagnosis, surgery, and treatment methods, GBM remains one of the most deadly cancers with a very poor outlook [Carrasco-Garcia et al., 2014]. The average survival time after treatment is between 12–17 months [Gramatzki et al., 2016, Stupp et al., 2005], but without treatment, it falls to around 6.1 months [Markert, 2003]. The two-year survival rate is approximately 26–33% [Stupp et al., 2015], and the five-year survival rate for primary GBM is very low, reported at 2.2% from a single centre in France in 2024 [Aboubakr et al., 2024]. Efforts to improve these outcomes have not led to significant progress [Weller et al., 2017], highlighting the need for large, multi-centre clinical trials to explore new treatment options.
GBM is highly aggressive due to its invasive growth, varied genetic makeup, and resistance to standard treatments [Tan et al., 2020]. The tumour cells spread widely into nearby healthy brain tissue, causing invasive growth and nearly always recurring, often within 2 centimetres of the original surgical site [van Rensburg and van Rensburg, 2012]. This makes GBM a “whole brain” or “whole CNS” disease, making complete tumour removal very difficult [Faustino et al., 2020]. Despite strong multi-treatment approaches, almost all patients face tumour recurrence [Auffinger et al., 2012, Bradshaw et al., 2016]. Treating recurrent GBM is especially hard, as there are no clear standard guidelines [Bajaj et al., 2024].
Several factors contribute to the poor prognosis due to the ineffectiveness of current GBM treatment, including:
Diffuse Infiltration of GBM cells into important brain areas makes complete surgical removal difficult. Maximal safe resection is a key part of GBM treatment, aiming to reduce tumour size and ease symptoms [Stupp et al., 2005]. Research shows that removing more of the tumour improves survival, but the benefits lessen when there is a risk of causing neurological problems after surgery [Lacroix et al., 2001]. The cancer cells spread along white matter paths and blood vessels, often several centimetres from the primary tumour [Scherer, 1940].
These cells go beyond the resolution of current neuro-imaging tools, making it hard to identify exact tumour edges before or during surgery [Galldiks et al., 2024]. As a result, fully removing the tumour is nearly impossible without causing significant brain function damage, as the infiltrating cells are in critical brain areas [Sanai and Berger, 2008].
Remarkable Resistance is shown by GBM to standard treatments such as chemotherapy and radiation therapy [Carrasco-Garcia et al., 2014]. This resistance is partly due to some GBM cells being located in areas of the tumour with low oxygen and tissue death [Klinz et al., 2011].
The Blood-Brain Barrier (BBB) and the natural resistance of glioma cells [Fortin, 2012] create a major barrier to effective treatment, reducing the delivery and impact of chemotherapy drugs [Arvanitis et al., 2020, Kesari, 2011, King and Benhabbour, 2021]. Although the BBB is partly disrupted in GBM, the blood-tumour barrier still blocks many chemotherapy drugs from reaching the tumour in high enough amounts. Additionally, invasive tumour cells at the edges are protected by an intact BBB [Markert, 2003].
Therapeutic Challenges arise from the wide variation in GBM at multiple levels, leading to treatment resistance and tumour recurrence [Sottoriva et al., 2013]. This variation in physical traits adds to the extensive genetic differences, increasing the tumour’s aggressiveness and creating significant barriers to effective treatment [Robertson et al., 2019].
Unknown underlying mechanisms complicates the development of targeted therapies. GBM cells show increased ability to move, driven by changes in cell adhesion molecules, extracellular matrix components [Giese et al., 1996], and signalling pathways like integrins, Matrix Metalloproteinases (MMPs)s, and the Phosphatidylinositol 3-Kinase (PI3K)/Akt pathway [Nakada et al., 2007]. The tumour micro-environment, including low oxygen levels and interactions with surrounding cells, also encourages invasive behaviour [Charles et al., 2011].
Radiotherapy: an Essential Component#
In the standard treatment protocol, RT is essential for managing tumour growth and improving patient survival. Complete surgical removal is not feasible due to the tumour’s invasive characteristics [Sanai et al., 2011]. Therefore, post-operative RT targets remaining tumour cells in the resection cavity and nearby brain tissue [Lawrence et al., 2012] to lower the chances of local tumour recurrence. RT employs high-energy ionizing radiation from the electromagnetic spectrum and can be delivered with four purposes: (i) curative: to eliminate cancer, often combined with chemotherapy; (ii) adjuvant: to support surgery and reduce the risk of tumour recurrence; (iii) palliative: to alleviate symptoms and improve patient comfort; and (iv) neo-adjuvant: to shrink tumours before surgery, such as in rectal cancer [Vaidya, 2021].
The core principle of RT lies in selectively targeting cancer cells while preserving healthy cells. Cancer cells often exhibit impaired DNA repair mechanisms, making them unable to recover from RT-induced DNA damage. In contrast, healthy cells can repair such damage to a certain extent. However, exceeding a tissue-specific threshold of ionizing radiation can overwhelm the repair capacity of normal cells, potentially leading to secondary cancers where healthy cells become malignant [Newhauser and Durante, 2011]. To mitigate the risks of normal tissue toxicity, a stringent radiation protection framework, encompassing laws, procedures, and regulations, is essential to minimize these hazards.
RT is typically administered using photons or other charged particles [Durante and Loeffler, 2010]. Photon-based therapy employs high-energy X-rays that penetrate deeply into body tissues while minimizing damage to the skin surface. These X-rays generate secondary electrons that disrupt DNA in both cancerous and healthy cells [Jakob et al., 2009]. Both photon and electron therapies rely on a Linear Particle Accelerator (LINAC) for precise delivery. Proton therapy is increasingly utilized, particularly for paediatric cases and brain tumours, due to its ability to deliver radiation with minimal impact on surrounding healthy tissues [Durante et al., 2017]. However, challenges include its high cost, limited availability, and insufficient clinical evidence demonstrating clear advantages over other methods in many adult cancers [Loeffler and Durante, 2013]. Unlike photons, which travel through the body in near-linear paths, protons can be targeted to deposit energy locally, sparing tissues beyond the tumour site.
Treatment planning for GBM is complex due to the difficulty of defining Target Volume (TV) that include all infiltrative tumour cells while minimizing toxicity to healthy brain tissue [Paulsson et al., 2014]. To address microscopic disease, margins are typically extended beyond (called the Clinical Target Volume (CTV)) the visible tumour (called the Gross Tumour Volume (GTV)) on imaging studies, but this method lacks precision and may fail to encompass all infiltrative cells while exposing normal tissue to radiation [Minniti et al., 2010]. The diffuse infiltration of GBM into surrounding brain tissue, often beyond what conventional imaging can detect [Giese et al., 2003], poses significant challenges for radiation oncologists in accurately delineating the tumour. This ambiguity complicates the use of automated tools, which may struggle to differentiate tumour tissue from normal brain tissue, potentially underestimating tumour volume [Akkus et al., 2017]. Unclear margins reduce the precision of RT targeting. Both conventional approaches and emerging AI models designed to enhance treatment planning must account for the microscopic spread of tumour cells [Niyazi et al., 2012], a task made difficult by the lack of clear imaging markers.
Current imaging modalities, such as MRI and Positron Emission Tomography (PET), are limited in their ability to detect microscopic tumour infiltration [Galldiks et al., 2024]. Advanced techniques, including Diffusion Tensor Imaging (DTI) and Magnetic Resonance Spectroscopy (MRS) [Price et al., 2003], provide greater sensitivity but are not commonly used in clinical settings due to economic, technical, and interpretive challenges. The difficulty in precisely identifying the full extent of tumour infiltration complicates effective surgical planning and accurate RT targeting.
Workflow Challenges#
The foundation of effective radiation therapy is meticulous treatment planning. This section addresses two primary challenges in this process, which form the motivation of the research objectives explored throughout this thesis. Treatment planning commences with the acquisition of medical images, such as Computed Tomography (CT), PET, and MRI, capturing the patient’s anatomy. These images form the backbone for contouring or delineation, where TV, encompassing the tumour and areas at risk for microscopic disease, and Organ at Risk (OAR) are carefully outlined [Dawson and Sharpe, 2006].
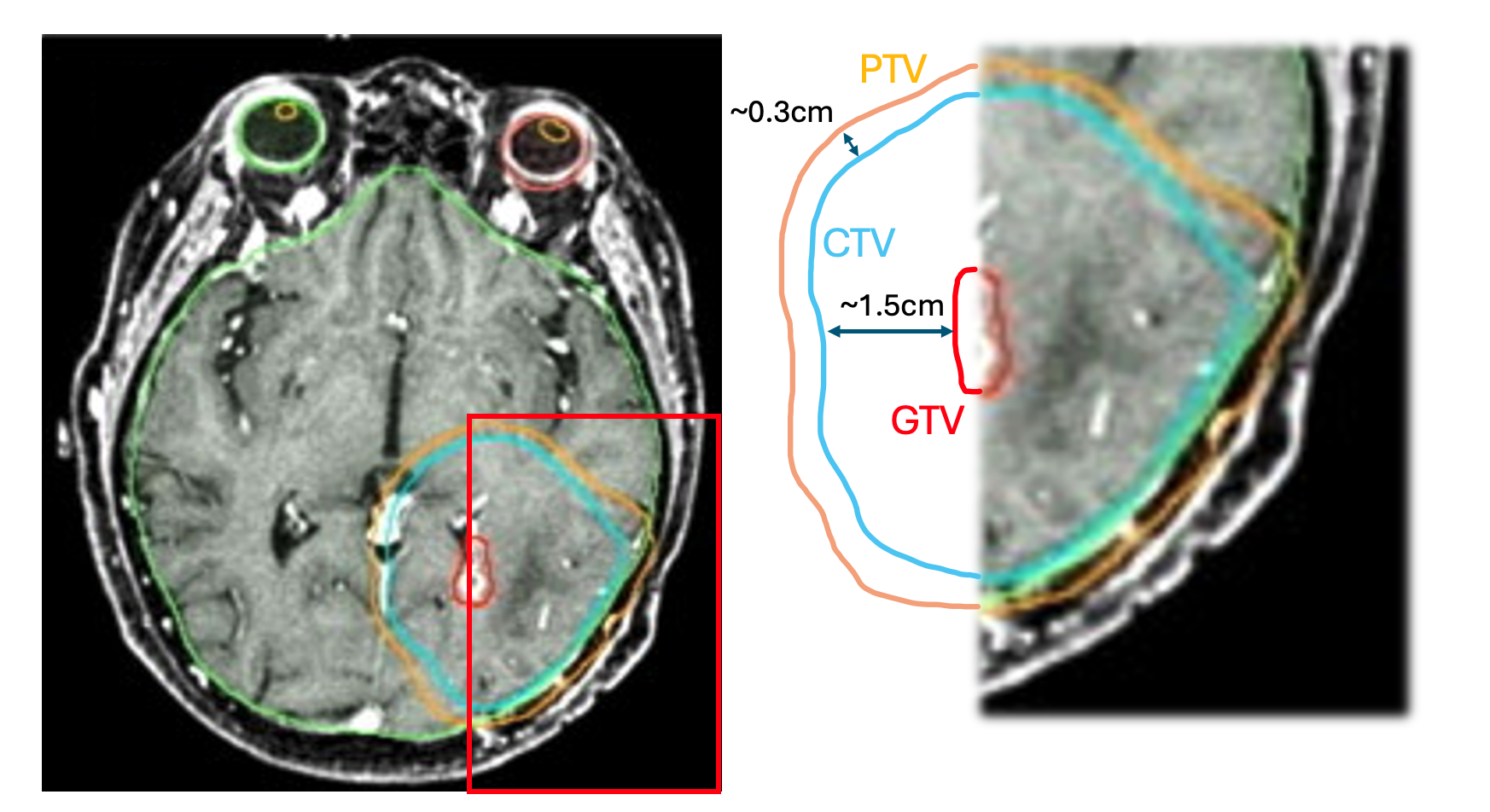
Typical situation in contouring, where the OARs like the eyes are delineated. Zoomed in section (in red) on the right shows the guidelines for TVs from [Niyazi et al., 2023], indicating typical extensions of the GTV to form the CTV and then the Planning Target Volume (PTV).#
Manual contouring is typically performed by radiation oncologists or dosimetrists using specialized software to delineate structures slice-by-slice on medical images. This task demands extensive anatomical knowledge, clinical expertise, and careful interpretation of imaging features. The resulting contours guide medical physicists in developing treatment plans that deliver the prescribed radiation dose to the TV while minimizing exposure to healthy OAR tissues [Wu et al., 2017]. Accurate contouring is critical, as it directly impacts treatment outcomes. Errors in contouring can result in geographic miss of the TV, leading to under-dosing of the tumour, or excessive irradiation of healthy OAR tissues, causing toxicity. Despite standardized guidelines and protocols [Niyazi et al., 2023], manual contouring remains heavily reliant on human judgment, leading to considerable inter- and intra-observer variability, which poses a significant challenge in RT planning [Podobnik et al., 2024]. elaborates on these challenges and discusses current advancements in automation to address them.
The subsequent phase of treatment planning employs advanced techniques such as IMRT and Volumetric Modulated Arc Therapy (VMAT), which involve a highly iterative process heavily reliant on manual input. Treatment planners undertake multiple trial-and-error iterations to balance the competing goals of effective tumour control and the preservation of healthy tissue [McIntosh et al., 2016]. This process requires repeated adjustments to planning parameters, dose constraints, and optimization objectives until a clinically acceptable plan is achieved [Djajaputra et al., 2003, Kajikawa et al., 2019]. provides a detailed examination of the challenges associated with this step, which leads to the core problem statement of this thesis, further discussed.
Variability in Contouring Practice#
Manual contouring in RT treatment planning is prone to significant variability, which presents in two main forms: inter-observer variability, arising from differences among clinicians, and intra-observer variability, stemming from inconsistencies in repeated contouring by the same clinician [Simões et al., 2019]. This issue is substantial, as inter-observer variability in TV contouring can exceed errors in other stages of the treatment planning and delivery process [Njeh, 2008, Segedin and Petric, 2016]. Such variability may introduce systematic errors in dose delivery, potentially compromising local disease control [Baroudi et al., 2023]. The factors contributing to contour variability.
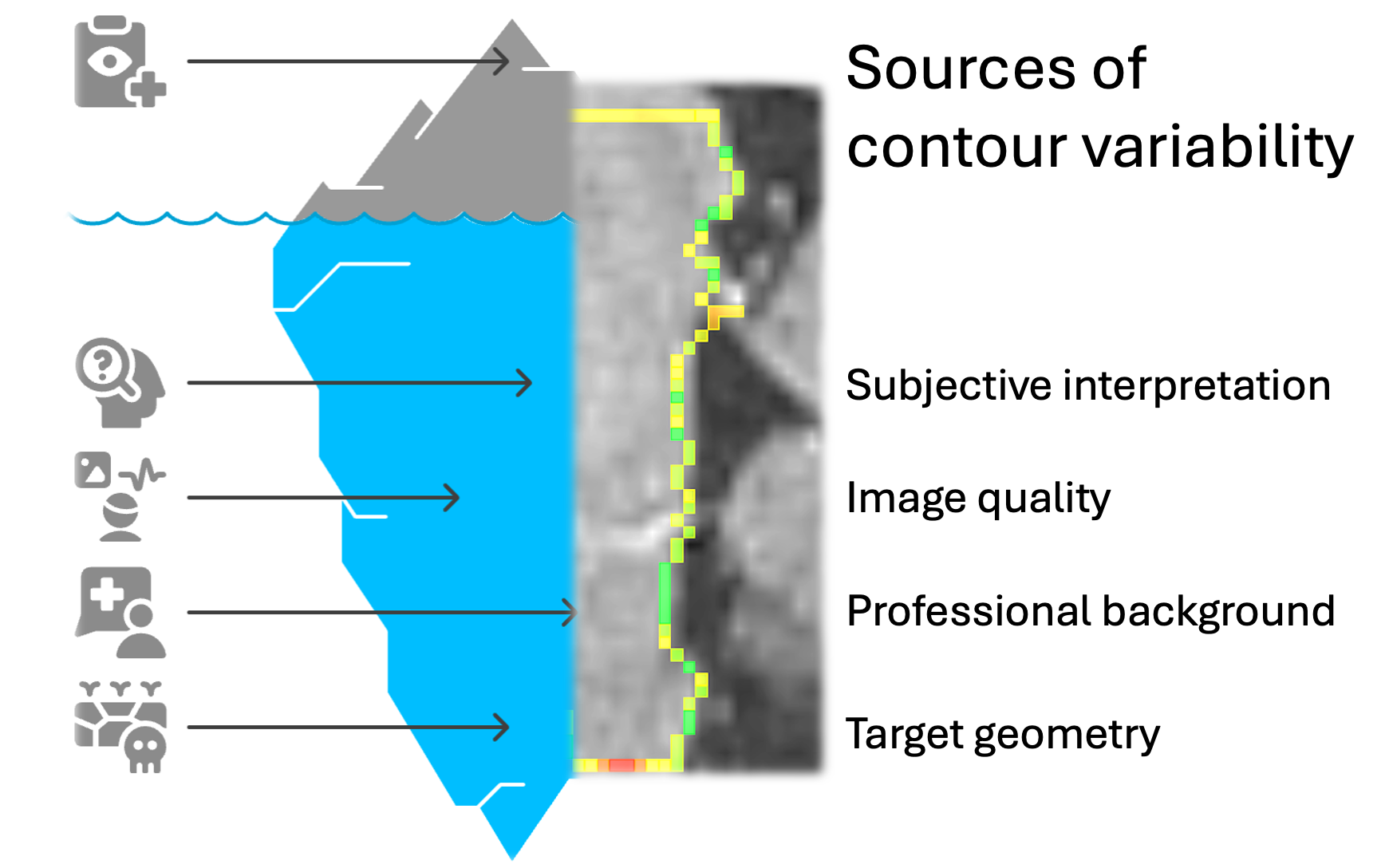
The various causes of contour variability are described in this iceberg representation. Right half of the figure represents an example of contouring variation (green: consistent, red: deviation) between three expert radiation oncologists for the brainstem contour, overlaid on the T1c image data, used to determine the boundaries.#
Sources of variability: The causes of contour variability in RT treatment planning are complex and diverse. A primary factor is the subjective interpretation of anatomical boundaries, particularly in regions with limited tissue contrast [Zhu et al., 2019]. This challenge is pronounced in tumours where soft tissue boundaries are obscured by motion or poor contrast with adjacent OARs [Kirby et al., 2025]. For instance, studies on pancreatic tumours have demonstrated significant discrepancies, with ratios of the largest to smallest delineated GTV within the same patient reaching as high as 6.8 [Versteijne et al., 2017].
Image quality plays a critical role in contour accuracy, with artifacts, calcifications, and motion blur contributing to increased variability [Nelson et al., 2023]. Certain anatomical structures pose greater challenges than others. Organs such as the lungs and bladder, which have well-defined boundaries, allow for consistent delineation. In contrast, structures like the parotid glands and small bowel, with less distinct borders, result in greater interpretive variability [Mercieca et al., 2020]. For example, studies have reported significant variations in contouring cardiac structures, particularly the Left Anterior Descending Artery (LAD), due to its poor visualization on non-contrast CT scans [Arculeo et al., 2020]. Additionally, the background and level of experience of the individual performing the contouring significantly influence variability [Attard and Mercieca, 2024]. Differences are observed not only among various healthcare professionals, such as radiation oncologists, dosimetrists, or radiologists, but also among clinicians with differing levels of training [Das et al., 2021].
The complexity of target geometry significantly increases contouring challenges, particularly when tumours exhibit intensity levels similar to surrounding tissues [Chebrolu et al., 2014]. Consistent difficulties arise in areas such as the longitudinal extent of head and neck cancers, tumours adjacent to consolidated lung tissue or potentially invading the mediastinum [Apolle et al., 2019], regions near biliary stents or suspicious lymph nodes [Versteijne et al., 2017], and structures affected by motion, such as thoracic regions influenced by respiration [Kirby et al., 2025]. The impact of this variability is substantial. As treatment techniques like IMRT become more conformal, variations in manual contouring can lead to critical errors, resulting in geographic miss of TV or excessive irradiation of OARs [Velker et al., 2013, Özsavaş et al., 2014]. Moreover, contouring inconsistencies hinder the standardization of patient treatments across different centres and clinicians [Brouwer et al., 2012].
Current Research Directions: To address contouring variability, the field has increasingly adopted automated contouring solutions, which offer notable advantages. A key strategy involves developing and applying standardized anatomical guidelines and contouring atlases [Niyazi et al., 2023, Niyazi et al., 2016]. These resources provide clear delineation protocols to improve consistency among radiation oncologists. Furthermore, Quality Assurance (QA) sessions and specialized training have been identified as essential for reducing inter-observer variability and standardizing TV delineation across clinical settings [Cardenas et al., 2022]. Despite these efforts, guideline-based approaches alone have not fully resolved variability [Turcas et al., 2023], prompting increased focus on automated contouring solutions.
Auto-contouring technologies have developed along two main pathways: traditional atlas-based methods and modern AI approaches, particularly Deep Learning (DL) [Han, 2011]. Atlas-based auto-segmentation has demonstrated success in reducing workload, but it often necessitates substantial manual adjustments to meet clinical standards [Cavus et al., 2024]. Research indicates that less experienced physicians experience greater reductions in contouring time compared to their more experienced counterparts [Chao et al., 2007].
AI approaches have demonstrated significant time efficiency, reducing total contouring workflow time by up to 80 minutes (65%) in head and neck anatomy, with smaller time savings in other anatomical regions [Radici et al., 2022]. Multiple studies have shown that computer-assisted contouring methods substantially decrease inter-observer variability [Hu et al., 2023]. This enhanced consistency is particularly beneficial for standardizing treatments across various centres and clinicians, thereby improving the reliability of clinical trial data [Zhang et al., 2022]. As these technologies advance, integrated strategies combining standardized guidelines, QA processes, and advanced auto-contouring tools offer the most promising approach to tackling the ongoing challenge of contouring variability in RT planning [da Silva et al., 2018, Lin et al., 2021].
Limitations of Current Approaches: Despite these advancements, most auto-contouring systems still require manual review and editing [Rasmussen et al., 2024]. They are increasingly regarded as valuable tools that provide a starting point to reduce workload and enhance consistency, rather than fully replacing clinical expertise [Radici et al., 2022]. Evaluating the performance of these automated systems is a critical area of ongoing development. Common evaluation methods include geometric metrics such as the Dice Similarity Coefficient (DSC), Hausdorff Distance (HD), and other measures of overlap and distance [Cao et al., 2020, Sharp et al., 2014, Taha and Hanbury, 2015]. These metrics assess the accuracy of auto-generated contours against manually defined gold standards. However, research suggests that geometric metrics often do not strongly correlate with dosimetric outcomes, which are closer to estimating clinical impact [Poel et al., 2021].
Time-consuming Plan Optimization#
The manual method used for treatment planning has several important limitations. One of the main issues is that it is highly time-intensive, often requiring planners to spend many hours or even several days on a single patient case [Rago et al., 2021, Wang et al., 2019]. This challenge is even greater in cases involving complex areas of the body, such as head and neck cancer. In these situations, planners must consider multiple target dose levels and many nearby OARs, which makes the process especially difficult and time-consuming [Li et al., 2020, Liu et al., 2023].
The quality of a treatment plan depends greatly on the expertise and experience of the planner [Wang et al., 2020, Zarepisheh et al., 2022]. Creating an effective plan requires a deep understanding of what the Treatment Planning System (TPS) can and cannot do, along with the ability to estimate what kind of dose distribution is realistic for each patient [Krayenbuehl et al., 2015, Nwankwo et al., 2015]. Because this process relies so much on human judgement, there can be a lot of variation in the quality of plans, even among planners working in the same clinic [Gintz et al., 2016, Phurailatpam et al., 2023]. Treatment planning also involves multiple stakeholders, such as radiation oncologists, medical physicists, and dosimetrists [McIntosh et al., 2016]. Coordinating between these professionals adds complexity to the workflow. For example, treatment plans often go through several rounds of review and revision based on feedback from oncologists, which can take extra time [Liu et al., 2021]. This teamwork, although essential, can lead to delays, especially in urgent cases where time is limited [Gao et al., 2024].
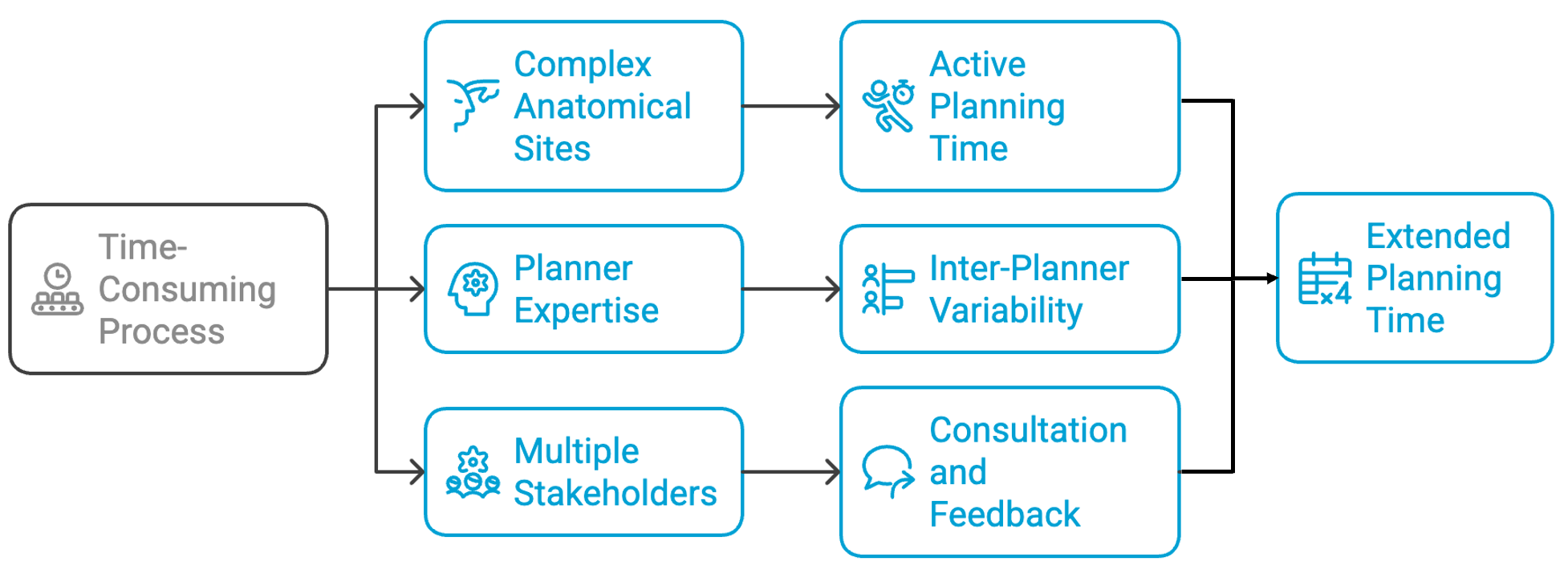
Why is the current workflow of treatment planning time consuming? Here are three common factors that lead to excessive delays in generating acceptable treatment plans.#
For complex treatment sites, such as head and neck cancer, the planning process is particularly challenging due to the non-convex geometry of TVs and their close proximity to critical structures [Li et al., 2020]. Advanced techniques, such as IMRT, enable highly conformal dose distributions but require significantly more complex and time-intensive planning [Arbea et al., 2010, Bohara et al., 2020, Webb, 2003]. The manual and iterative nature of treatment planning further reduces clinical efficiency and may affect treatment outcomes. Due to time constraints in clinical practice, compromises are sometimes necessary, which can lead to suboptimal plans being used in treatment [McIntosh et al., 2016, Sayre and Ruan, 2014]. This underscores the conflict between achieving high-quality plans and maintaining efficiency in demanding clinical settings [Korreman et al., 2020].
Planning Time Requirements: The time demands of RT treatment planning for various treatment techniques and anatomical sites have been the focus of many past research projects. For example, active planning time for ten cases of glioblastoma (GBM) and pancreatic cancer using standard IMRT was reported to average around 135 minutes per case [Craft et al., 2012], highlighting the need for automation. In brachytherapy, especially for cervical cancer, the contouring and planning phases are particularly time-consuming, often taking about 3 hours on average [Fionda et al., 2024]. The planning process for techniques such as VMAT is also resource-intensive. A single optimization cycle can take up to 10 minutes using modern computing systems, and multiple iterations are usually needed to reach a clinically acceptable plan [Bice et al., 2021, Tian et al., 2015]. For Naso-Pharyngeal Cancer (NPC) cases, even experienced planners using conventional algorithms may require several hours to complete a single plan [Ng et al., 2021]. In general, complex treatment sites often demand several hours of work per plan [Gao et al., 2025]. This extended planning time poses a significant barrier to the wider adoption of adaptive RT, where plans must be updated frequently based on changes in patient anatomy [Antico et al., 2019, Cilla et al., 2021].
Causes for Long-computation Time: The complexity of RT treatment planning is driven by several interconnected factors that can extend the time from initial simulation to the first treatment session to several days or even weeks [Yu et al., 2022]. Modern treatment techniques such as IMRT and VMAT are now widely used because they offer better target coverage and improved protection of healthy tissues. However, these methods also make the planning process much more complex and time-consuming [van Gysen et al., 2020]. These advanced techniques produce highly detailed dose distributions, with each small segment of the radiation beam (beamlet) having a different intensity. As a result, the planning process requires significant computational power and close attention from the planner [Soh et al., 2019]. Moreover, when IMRT plans become too complex, they can lead to increased uncertainty in dose delivery, longer treatment times, and greater sensitivity to any changes in the patient’s anatomy or position [Du et al., 2014].
The iterative trial-and-error approach commonly used in treatment planning becomes especially difficult when dealing with complex anatomical sites. Planners often need to create and evaluate several versions of a plan before reaching one that meets clinical standards. This process can take a significant amount of time, even for experienced medical physicists [Fan et al., 2018, Xia et al., 2021]. The workload is further increased by the growing need for detailed documentation, the introduction of new technologies, a wider range of available treatment options, and stricter regulatory QA requirements. Each of these factors adds additional steps to the planning process, increasing both the time and effort needed for each individual case [Ahmad et al., 2020].
The quality of treatment plans depends strongly on the skill, experience, and available time of the planner during the optimization process [Heilemann et al., 2025]. Because of this reliance on individual expertise, there can be significant variation in both the quality and efficiency of treatment plans, which may affect patient outcomes. As the demand for RT services continues to grow, many clinics face increasing pressure on their planning resources. This often leads to a conflict between the goal of delivering high-quality, personalized treatment plans and the practical limitations of a busy clinical workflow [Cozzi et al., 2019].
These planning challenges have important consequences in certain clinical situations. In palliative care, where the main goal is to relieve symptoms quickly, delays in treatment planning can be particularly harmful. Standard simulation and immobilization procedures may also be difficult to apply in patients who are medically fragile or have complex health conditions [Dyer et al., 2019]. Furthermore, the time-consuming nature of current planning methods creates major bottlenecks that limit the progress of personalized and adaptive RT, especially techniques such as online treatment adaptation that require rapid plan generation [Qiu et al., 2023].
The continued reliance on manual inputs and standardized protocols in the RT workflow, while generally effective, is increasingly challenged by patient-specific variability. As treatment cases become more complex and clinical demands grow, these traditional approaches may no longer provide optimal efficiency or consistency [Wildman et al., 2024]. In response to these limitations, there has been growing interest in automated planning techniques. These methods are especially promising for complex treatments that involve advanced modalities and intricate target geometries, where manual planning can be particularly time-consuming and variable [Marrazzo et al., 2023].
Impact on Care: The significant time required for RT planning presents major challenges in how clinical departments allocate resources, directly affecting patient care in several important ways.
Delays in planning can result in longer intervals between simulation and the start of treatment, which have been associated with worse survival outcomes [Peters et al., 2010, Shen et al., 2012]. These delays also contribute to increased workload pressures, especially as cancer incidence rises, making manual scheduling more complex and time-consuming [Vieira et al., 2021]. This issue is particularly critical in palliative cases, where rapid symptom relief is essential and patients may not tolerate standard simulation or immobilization techniques due to their medical condition [Dyer et al., 2019]. In many cases, limited planning resources force a trade-off between delivering high-quality, individualized treatments and managing the day-to-day demands of a busy clinic [Cozzi et al., 2019]. When faced with high patient volumes and time constraints, clinicians may have no choice but to proceed with suboptimal plans, which can negatively affect treatment quality. This is especially concerning given the well-documented link between adherence to RT protocols and improved treatment outcomes [Anand et al., 2021].
Efforts to Introduce Automation: The labour-intensive nature of current treatment planning processes often require several hours or even days per case, and has led to growing interest in automation and AI as potential solutions to reduce planning time [Nardone et al., 2024]. These technologies offer the opportunity to streamline workflows and improve clinical efficiency without compromising plan quality. For instance, automatic VMAT planning could help overcome a major bottleneck in clinical practice. Recent advancements in planning technology have shown promising results, with some systems capable of generating high-quality prostate treatment plans in just 7–15 minutes. This level of speed could make real-time adaptive RT which was once considered impractical to be feasible in routine clinical workflows [Cilla et al., 2021].
Personalized planning engines have achieved impressive reductions in overall planning time, including human inputs, optimization processes, and calculation times. Personalized approaches have reduced planning times to 60-80 minutes, approximately one-third of the time needed for manual planning [Cilla et al., 2020].
Automated treatment planning pipelines are being developed to produce plans of comparable quality to those generated manually, but without requiring the several hours of labour per plan typically needed for conventional approaches [Gao et al., 2025]. These systems aim to improve efficiency while maintaining or enhancing plan quality consistency [Bellotti et al., 2024].
Online adaptive planning methods leverage automation to enable real-time plan adaptation while patients are on the treatment couch. The dramatic reduction in planning time achieved through automated approaches opens new possibilities for implementing adaptive RT strategies that were previously impractical due to time constraints [Cilla et al., 2021, Qiu et al., 2023].
Knowledge-based planning models have demonstrated remarkable efficiency improvements, with some studies reporting treatment planning time reductions of up to 95% [Júnior and Teixeira, 2023]. These approaches rely on data libraries built from prior treatments and planner-independent optimization algorithms to streamline the planning process, reducing reliance on manual trial-and-error iterations [Ng et al., 2021].
AI-based planning agents represent a future direction where planning can be efficient and effective with minimal human intervention [Nardone et al., 2024]. These approaches have particular potential for time-sensitive scenarios such as adaptive RT that requires frequent and rapid planning [Gao et al., 2024].
Unmet Clinical Needs#
The challenges listed in the previous section demonstrate the need for contour QA to be performed automatically and reliably. The widespread recognition of contouring variability has established QA and peer review as integral components of radiation oncology practice. Despite the existence of specific guidelines for OAR delineation in clinical practice and research, considerable inter- and intra-observer variations have been documented. These variations can lead to inconsistent dose evaluations, potentially compromising treatment efficacy and complicating toxicity analysis [Men et al., 2020]. A study with four radiation oncologists and three radiologists delineating parotid glands showed that inter-observer variation in contour delineation is significant enough that nearly half of reviewed contours would have resulted in different treatment plans if used clinically [Loo et al., 2012]. As auto-contouring becomes increasingly prevalent in clinical settings, QA remains crucial. Even as automated tools replace manual contouring in routine practice, quality checks still rely on clinicians [Nelson et al., 2023]. AI-generated contours typically require review and adjustment by radiation oncologists before treatment planning, emphasizing the complementary relationship between automated systems and human expertise [Hoque et al., 2023]. Automated approaches to contour review may decrease review time and improve consistency, making them valuable tools either stand alone or as assistants to human reviewers in identifying poor-quality contours [Brooks et al., 2024]. This section elaborates on this unmet clinical need, motivating the research aims in this thesis.
Current Approaches to Contour QA#
QA in general encompasses all procedures that ensure consistent and safe delivery of prescribed radiation doses to TVs while minimizing exposure to normal tissues and monitoring patient outcomes. This comprehensive process requires cooperation across all staff groups as the quality activities are interdependent throughout the RT workflow [Ismael and Hassan, 2020]. Contour assessment can be conducted both visually and quantitatively. While visual inspection remains the most common approach, it is time-consuming and subjective [Terparia et al., 2020]. QA in RT contouring encompasses a range of methods and approaches, like shown in Figure..
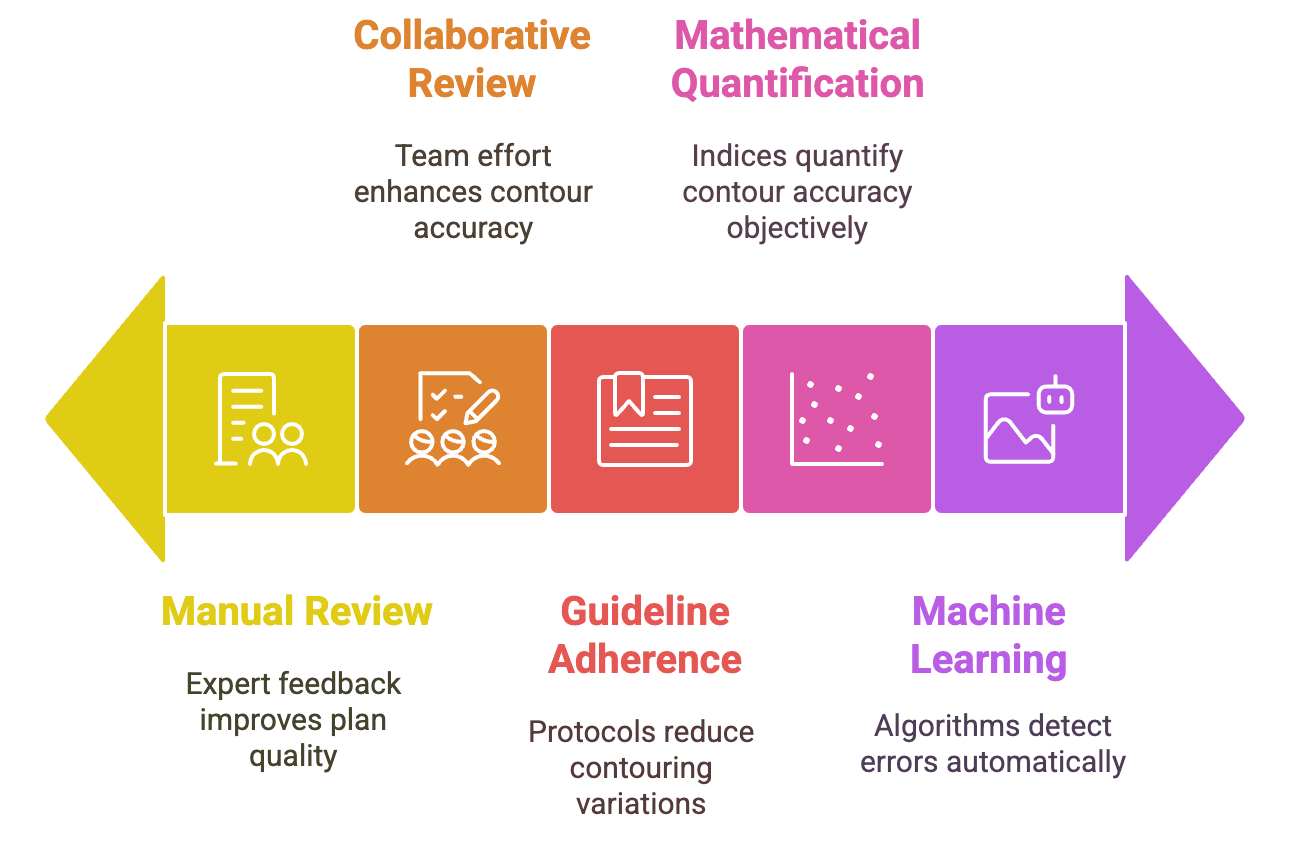
Current methods of contour QA spans the complexity spectrum from manual peer reviews and guideline-based adherence all the way up to machine learning methods. Figure generated using napkin.ai#
Peer Review: is a formal review by another expert of the delineated contours used to produce a RT plan, has become a critical mechanism for quality improvement [Lewis et al., 2020]. This process of traditional “chart rounds” involving contour review, radiation dose prescription scrutiny, and treatment plan evaluation has demonstrated significant clinical impact, with studies showing that peer review leads to changes in approximately one in nine radiation plans [Cooper et al., 2020]. Weekly teleconferences with radiation oncology specialists for detailed target and OAR review prior to treatment plan creation, with changes classified as “major” (modifications to high-dose PTV or prescription) or “minor” (modifications to intermediate/low-dose PTV or OARs) [Hughes et al., 2022]. From a survey among 115 radiation oncologists in the US, 44% reported performing a contour-specific peer review in their practice. Furthermore, 72% of these respondents reported that contouring-related questions arise in at least half of cases in routine patient care [Zhang et al., 2021]. Prospective contour and plan review with radiation oncologists and site specialists, along with secondary QA contour checks performed by trained dosimetrists or medical physicists during treatment has been reported [Teoh et al., 2023]. Weekly contouring QA meetings where radiation oncologist contouring is peer reviewed prior to dosimetric planning, have served as both quality control and educational forums for trainees [Nicholls et al., 2016].
Standardization Approaches: Consensus contouring guidelines and atlases have been used to reduce TV delineation variability [Chang et al., 2017]. A survey indicated that 75% of radiation oncologists first consulted cooperative group guidelines and contouring atlases (e.g., RadioTherapy Oncology Group (RTOG)/NRG Oncology (NRG)) when contouring questions arose [Zhang et al., 2021]. Institutional, national, or international protocols have also been shown to reduce intra- and inter-observer variation in TV delineation [Nicholls et al., 2016].
Quantitative Assessment Methods: Conformity Index (CI) used to mathematically quantify contour accuracy against gold standards, including: DSC, Jaccard Conformity Index (JCI), van’t Riet Index (VRI), Geographical Miss Index (GMI), Discordance Index (DI), HD [Li et al., 2016, Terparia et al., 2020], Protocol deviation scoring systems, commonly used in clinical trials, with standardized criteria: Score “1”: OAR contours acceptable with no edits, Score “2”: OAR contours acceptable with minor edits not likely to affect treatment plan, Score “3”: OAR contours unacceptable, requiring major edits likely to affect treatment plan [Zhang et al., 2022].
The quality of contour delineation has profound implications for treatment outcomes in RT. Inaccuracies in TV and OAR contour delineation directly impact both tumour control and normal tissue toxicities [Marquez et al., 2024, Nijhuis et al., 2021]. The clinical significance of this impact has been quantitatively demonstrated in multiple studies. For instance, research examining parotid gland delineation found that the Dose-Volume Histogram (DVH)s of 46% of study contours were sufficiently different from those used clinically that they would have produced different intensity-modulated RT (IMRT) plans [Loo et al., 2012, Men et al., 2020].
Motivating Dosimetric Contour QA#
The dosimetric impact of contouring errors is particularly significant with advanced RT techniques. The highly conformal nature of modern treatment modalities increases the dosimetric impact of delineation errors, making contour QA increasingly important [Nijhuis et al., 2021]. This is especially true in anatomical regions like the head and neck, where the therapeutic window is narrow due to the proximity of PTV to OAR [Buciuman and Marcu, 2021, Marquez et al., 2024]. Despite the critical importance of contouring accuracy, research has found that while 99.1% of studies presenting auto-contouring models report geometric agreement metrics, only 23.1% report the resulting dosimetric impact, which is essential for understanding the clinical consequences of contouring errors [Mackay et al., 2023]. This disconnect between geometric evaluation and clinical impact assessment highlights a significant gap in this research space, leading to the motivations for this work.
Automated QUality Assurance (AQUA) systems have emerged as critical tools for RT, offering methods to systematically detect contouring errors that may impact treatment outcomes. These systems employ various approaches to evaluate contour quality without requiring extensive manual review. Machine learning-based error detection methods extract geometric features of OARs and apply classification algorithms to identify contours that deviate from expected parameters [Chen et al., 2015]. Image feature-based conditional random forest algorithms approaches have been developed for different anatomical sites, with researchers using image features for thoracic structures, principal component analysis for pelvic structures, and surface-based metrics for female pelvis contours [Rhee et al., 2022] tolerances of 1-3 mm for detecting contouring errors with accuracy higher than 0.9 for most targets and critical structures have been reported to be used for automating these checks [Rhee et al., 2019].
DL techniques are increasingly being employed for automatically assessing contours, with recent work exploring deep active learning for OAR [Men et al., 2020] and an intelligent DSC threshold based quality control system [Luan et al., 2023]. A secondary segmentation algorithm to help classify errors in the primary model has been developed with promising classification accuracy and recall [Claessens et al., 2022]. Studies implementing DL-based contour models for OARs have shown significant time savings while maintaining or improving contour quality. In one study, total contouring time was reduced by 76% with radiation oncologist revision time specifically reduced by 35% compared to traditional workflows [Lucido et al., 2023]. Novel approaches are being developed to not only detect but also correct contouring errors. An automated QA and adaptive optimization correction strategy has been proposed that can identify incorrect auto-contours, provide potential error reasons and locations through attention heat maps, and use vision-language representations with convex optimization algorithms to adaptively correct problematic contours [Luan et al., 2024].
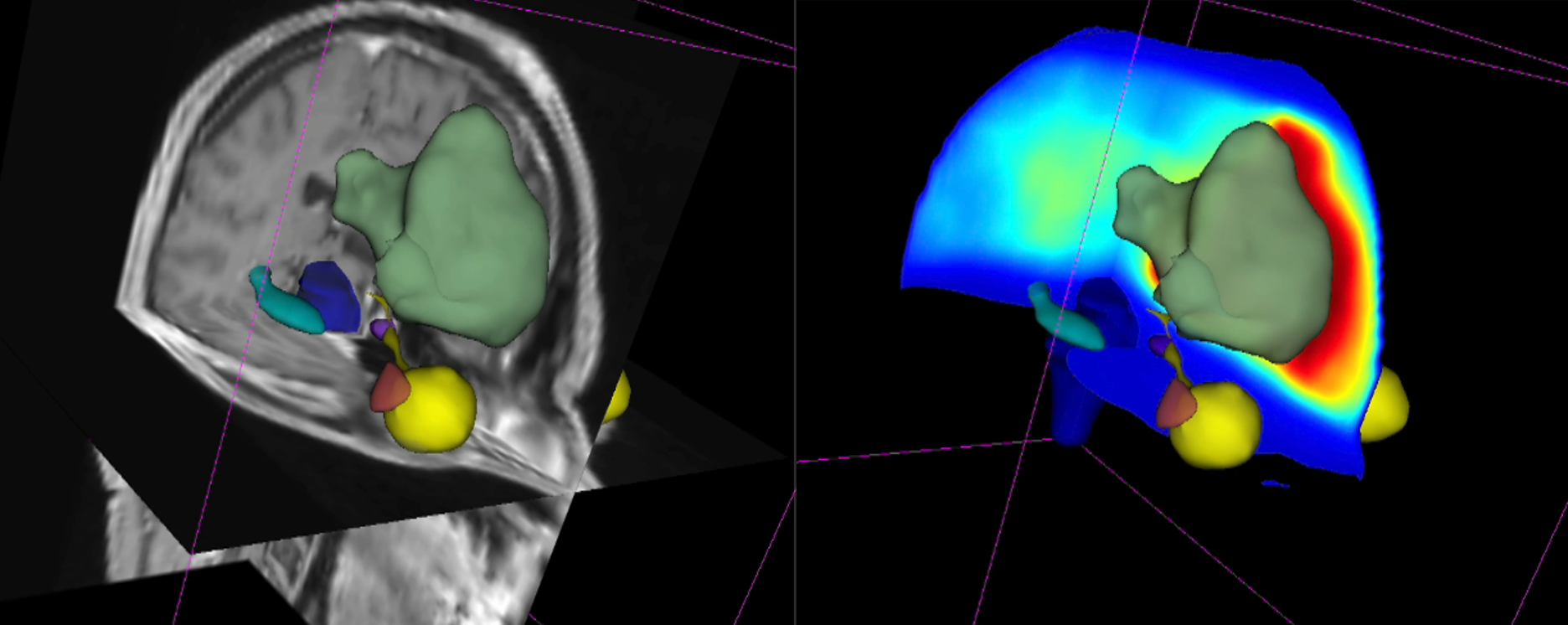
Motivating dosimetric QA: on the left: 3D slice plane and mask visualization for OARs and TV (in green) overlaid on T1c image data. On the right, the same overlaid on the dose distribution: hotter regions indicate higher dose, where accuracy of contours is arguably more important.#
In summary, there is an unmet clinical need for developing dosimetric tools for contour QA to streamline the workflow and provide fast and reliable feedback to clinicians. However, external validation of these QA approaches is essential before deployment to clinics with different patient populations and clinical practices [Netherton et al., 2025]. Automated approaches to contour review can decrease review time and improve consistency, making them valuable tools either on their own or as assistants to human reviewers in identifying poor-quality contours [Brooks et al., 2024, Duan et al., 2023, Rhee et al., 2022, Rhee et al., 2019, van der Veen et al., 2020, Wong et al., 2021]. The increasing adoption of AI tools in clinical practice has shifted the workflow paradigm. While auto-contouring is gradually replacing manual contouring in routine practice, quality checks still rely on clinicians [Nelson et al., 2023], and reviewing them in a dose-aware manner is gaining importance.
Hypothesis, Contributions, and Structure#
This work progresses from establishing the limitations of human dosimetric judgement to testing automated dose-aware assessment and ranking. It then examines whether the dose-prediction models that enable such assessment are sufficiently sensitive and robust, before investigating the robustness of the segmentation architectures on which auto-contouring and dose prediction depend. The two proof-of-concept tools are placed alongside the evidence from which they arise: AutoDoseRank in Part One and ASTRA in Part Two.
Hypothesis and Aims#
This leads to the central hypothesis of this work:
Fast, dose-aware AI systems can make contour QA in RT planning more consistent and clinically meaningful, provided that their dose-prediction and segmentation components are sensitive to consequential contour variations and robust to distribution shifts.
The hypothesis is examined through three groups of research questions that match the three parts of this site:
A: Dosimetric Awareness of Radiation Oncology Professionals: Is dose-aware automation needed, and can it improve contour assessment?
A1: How consistently can radiation oncology professionals estimate the dosimetric impact of contour variations?
A2: Can a deep-learning dose predictor identify dosimetrically sub-optimal contours as well as, or better than, expert reviewers?
A3: Can clinical dose criteria and organ-at-risk priorities be used to rank candidate auto-contours by dosimetric quality?
B: Sensitivity of Dose Prediction Models: Are dose-prediction models suitable for contour QA?
B1: Are their predictions accurate, fast, sensitive to realistic contour variations, and robust to out-of-distribution cases?
B2: Can their local sensitivity be converted into maps that focus review on the contour locations with the greatest dosimetric impact?
C: Robustness of Segmentation Models: How do model and data choices affect the reliability of the segmentation components used in this workflow?
C1: How do U-Net architecture choices, especially skip connections, interact with task complexity and robustness under texture shifts?
C2: How does the trade-off between image context and foreground ratio affect the performance and robustness of 3D segmentation networks?
This hypothesis and related questions are addressed in the following structure.
Research Contributions#
The subsequent chapters first quantify the gap between expert perception and dosimetric reality, then test automated assessment and ranking. They next evaluate dose predictors under realistic input variation and translate their sensitivity into a localized review tool. Finally, they examine how segmentation architecture and input sampling affect robustness. This three-part structure builds the case for practical AI-assisted contour QA while making the dependencies and limitations of the proposed workflow explicit.
Part One — Dosimetric Awareness of Radiation Oncology Professionals: This part motivates a shift from purely geometric to clinically meaningful dosimetric evaluation. The field has long relied on geometric metrics such as DSC for segmentation evaluation, yet these do not always correlate with clinical outcomes [Poel et al., 2021]. The contributions are:
Chapter 3 addresses A1 by measuring inter-expert variability in estimating the dosimetric impact of TV contour changes through a survey of seven clinical experts. This work was published in Radiotherapy and Oncology in 2025.
Chapter 4 addresses A2 through a head-to-head comparison showing that a DL dose predictor can outperform radiation oncologists in detecting dosimetrically sub-optimal contours. This work was presented as an oral talk at Medical Imaging with Deep Learning (MIDL) 2024.
Chapter 5 addresses A3 with AutoDoseRank, a dosimetry-informed framework that ranks TV contour candidates using dose constraints and clinical priorities. It outperformed three of four radiation oncologists in the reported triage task and was presented at the CaPTion workshop at MICCAI 2024.
Part Two — Sensitivity of Dose Prediction Models: After establishing the clinical need, this part examines the dose-prediction models used for automated dosimetric assessment. Such models can predict dose distributions rapidly [Liu et al., 2021], but their sensitivity and robustness must be validated for QA. The contributions are:
Chapter 6 addresses B1 with an extensive evaluation of sensitivity to OAR contour variations and robustness to out-of-distribution cases, including targeted data augmentation to mitigate observed failure modes. This journal study, published in Cancers in 2023, extends the conference work in Chapter 7.
Chapter 7 also addresses B1 by directly testing whether predicted dose changes track realistic inter-expert variation in OAR contours. This work was presented at the International Symposium on Biomedical Imaging (ISBI) 2023.
Chapter 8 addresses B2 and introduces Atomic Surface Transformations for Radiotherapy Quality Assurance (ASTRA), a method for visualizing where local OAR contour variations have the greatest impact on predicted dose. This work won the second-best student paper award at the Engineering in Medicine and Biology Conference (EMBC) 2023.
Part Three — Robustness of Segmentation Models: The final part examines U-Net-based architectures, which are ubiquitous in auto-contouring and dose-prediction pipelines [Azad et al., 2022], and asks how architecture and data choices affect reliability. The contributions are:
Chapter 9 addresses C1 by extending the Chapter 10 analysis across task complexities and texture variations. It finds that the value of skip connections is non-linear and context-dependent, and that more elaborate variants are not consistently more robust under distribution shift. This work was published in Computers in Biology and Medicine in 2025.
Chapter 10 provides the earlier conference study for C1, showing that skip connections offer their clearest benefit at high task complexity but can reduce robustness on out-of-domain clinical data. This work was presented at MICCAI 2023.
Chapter 11 addresses C2 by examining the trade-off between global image context and foreground ratio in 3D segmentation. It finds that attention-based and Transformer-based models are more sensitive to foreground-ratio shifts than a vanilla U-Net. This work was presented at the Medical Imaging meets NeurIPS workshop in 2022.
Thesis Structure#
The remainder of this thesis is structured as follows:
Part |
Chapters |
Theme and progression |
|---|---|---|
Background |
Chapter 2 |
Radiotherapy workflow, AI methods, and evaluation metrics used in the research chapters. |
Part One |
Chapters 3–5 |
Establishes variability in expert judgement, compares experts with automated dose prediction, and applies the result in AutoDoseRank. |
Part Two |
Chapters 6–8 |
Tests dose-prediction sensitivity and robustness, then applies local sensitivity in ASTRA. |
Part Three |
Chapters 9–11 |
Studies the robustness of segmentation architectures across skip-connection choices, task complexity, texture variation, context, and foreground ratio. |
Conclusions |
Chapter 12 |
Revisits the hypothesis, synthesizes the evidence, and discusses limitations and future validation. |
This organization is thematic rather than a strict technology-readiness sequence. In particular, the proof-of-concept systems are integrated into the parts that establish their foundations: AutoDoseRank follows the clinical-awareness studies in Chapter 5, while ASTRA follows the dose-sensitivity studies in Chapter 8.